Correspondence - Normal and Anomalous
Like last time, let's start off with a look at normal correspondence (NRC).
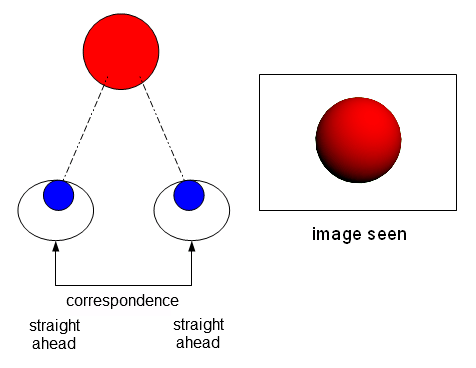
NRC exists when the brain believes that both eyes point straight ahead, in the same direction, at the same place. The two foveas are "hooked-up."
Like I said earlier, this correspondence works great when both eyes are actually pointing at the same thing. But if one eye is deviated, visual confusion and double vision result. Why? Because the brain still has that deeply ingrained belief that the two foveas correspond, that they look to the same place. (I'm using exotropia as an example, but the same would apply to esotropia.)

In most cases, the brain suppresses one eye to remedy this problem. The fovea-to-fovea correspondence remains intact.

Here's where it gets complicated. Instead of (or in addition to) suppression, the brain can alter the correspondence. Let's say that your left eye deviates 45 degrees outward. Your brain operates under the newer, more realistic assumption that your right fovea points straight ahead, and your left fovea points 45 degrees to the left. That is an abnormal or anomalous correspondence.
In the case of exotropia, this can lead to a widened, panoramic visual field. Instead two eyes operating binocularly to make one image, the two eyes operate monocularly to make one panoramic image, neatly joined in the middle.

Again, I'm not sure if an esotrope would see a panoramic view. I want to say probably not, but you never know. The brain is capable of many strange adaptations.
So that's the first problem of ARC. The foveas are not hooked up, and true fusion is not possible. The fovea of one eye doesn't overlap with the fovea of the other eye. It's the like story of the sun and the moon, of Apollo chasing Artemis. The sun approaches the moon, and the moon moves farther away. They're always separated by that 45 degrees of abnormal correspondence.
The second problem with ARC is that sometimes fusion and stereopsis DO happen, but in an abnormal and degraded way. This usually happens with a smaller angle of strabismus.
Clear, beautiful stereopsis happens with a fovea-to-fovea correspondence, because the foveas are the areas with the sharpest, clearest vision. But sometimes, someone with ARC will designate a new part of their retina to be a *new* fovea. A faux-fovea, you could say. They will then fuse the true fovea of one eye with the faux-fovea of the other eye. This can happen with in both esotropes and exotropes, and I have illustrated it in an esotrope below.

The true foveas are the green spots. As you can see, this person is using the true fovea of his right eye in conjuction with a faux-fovea (orange spot) of his left eye to create a fused image. The true fovea of his left eye isn't being used. It's just shooting off into nowhere.
If this were someone with normal correspondence, they would have reacted with double vision, visual confusion, or suppression. But this person is able to use both eyes together via a faux-fovea.
So what's the problem? Aren't they still getting some fusion and stereopsis? Yes, they are, and that's exactly what some optometrists and ophthalmologists say. Leave those poor ARC patients with fusion alone! Their angle of strabismus is usually so small as to not be noticeable, and they have some degree of fusion. The problem is that the fusion gained through a faux-fovea is of lower quality, and true binocularity is hard to achieve because the eyes have developed a very hard to break habit. It's also hard for the patient in vision therapy to know if they are successfully fusing with both foveas, or backsliding into ARC.
To sum up, these are the two problems of ARC. Number 1, the foveas are not "hooked-up", and chase each other like the sun and the moon, never able to overlap. Number 2, sometimes a faux-fovea develops in the turned eye, leading to some sort of low quality stereopsis, and that habit is hard to break.
How is ARC diagnosed?
I've read lots of ways to test for it, and I don't pretend to understand all of them. For instance, some involve using "troposcope or major amblyoscope", and I have no idea what those are. However, in general, these are the things that point toward ARC:
-Evidence of "pasting" the images from each eye into a panorama, such as wearing red/green glasses and seeing a half red / half green room. Or as I like to think of it, the sun chasing the moon.
-Diplopia "against the rule". I don't fully understand this, but apparently when inducing diplopia in a patient, the esotrope should generally see uncrossed diplopia, and an extrotrope should see crossed diplopia. If an exotrope saw uncrossed diplopia, for instance, that would be "against the rule" and point toward ARC.
-Evidence of fusion in someone who is clearly strabismic and deviating. If someone with crooked eyes sits down in an optometrists chair and shows evidence of fusion while the eyes are still crooked, the optometrist considers ARC. Why? Because they must be using a faux-fovea. When the angle of strabismus is not very noticeable, the optometrist can do a cover/uncover test while the patient is fusing, which would show if they are fusing while being out of alignment.
-An ARC result on the Bielschowski Afterimage Test. This was the camera flash test that I mentioned in the previous post. You flash the fovea of each eye, one eye horizontally and one eye vertically. If they afterimages line up, it shows a fovea-to-fovea correspondence. If they don't, then this points toward ARC.

Should ARC be treated?
There are many differing opinions on if ARC should be treated at all. Here's what I have found:
-Don't try to fix it. It's dangerous to try and can cause permanent double vision. I've only read this in relation to ophthalmology, though. I've also read the same thing about treating suppression. Apparently everything is dangerous except cutting into your eye with a knife.
-Don't try to fix it, because it's too deeply ingrained and can't be fixed.
-Try to fix it, but if the patient looks good cosmetically and is a good faux-fuser, then maybe it's not worth the trouble.
-Try to fix it, but be aware that it can take a long time and is not always successful.
-Don't try to fix it. It's dangerous to try and can cause permanent double vision. I've only read this in relation to ophthalmology, though. I've also read the same thing about treating suppression. Apparently everything is dangerous except cutting into your eye with a knife.
-Don't try to fix it, because it's too deeply ingrained and can't be fixed.
-Try to fix it, but if the patient looks good cosmetically and is a good faux-fuser, then maybe it's not worth the trouble.
-Try to fix it, but be aware that it can take a long time and is not always successful.
What is the treatment for ARC?
There are also many differing opinions on how to treat ARC. These are the methods I have come across:
-Start vision therapy with a STRONG emphasis on monocular training. Both eyes are trained separately, and the amblyopic / strabismic eye is exercised until it is equal in skill as the strong / fixating eye. This includes tracking, pursuits, and saccades. The exercises also include doing things like threading needles or stabbing Cheerios with a pencil, until YOU are able to do it equally well using either eye. This is supposed to orient each eye to the reality of the world, to make the eyes equal to each other (or close), and to show that both eyes correspond to the same reality. Visually directed movement activities can show the brain how the visual system lines up with reality.
-Bi-ocular tasks, such as anaglyphic (red/green) activities, that force fusion of the entire visual field. Touching and putting your hands on whatever you're looking at helps, too, and "proves" to your brain that each eye really does correspond in the same direction and to the same space.
-Dr Greenwald has a method of using prisms to cause diplopia in ARC. I gathered that the reason is to show the brain that the ARC adaptation isn't going to work anymore, and that a new correspondence must be developed (NRC).
-Start vision therapy with a STRONG emphasis on monocular training. Both eyes are trained separately, and the amblyopic / strabismic eye is exercised until it is equal in skill as the strong / fixating eye. This includes tracking, pursuits, and saccades. The exercises also include doing things like threading needles or stabbing Cheerios with a pencil, until YOU are able to do it equally well using either eye. This is supposed to orient each eye to the reality of the world, to make the eyes equal to each other (or close), and to show that both eyes correspond to the same reality. Visually directed movement activities can show the brain how the visual system lines up with reality.
-Bi-ocular tasks, such as anaglyphic (red/green) activities, that force fusion of the entire visual field. Touching and putting your hands on whatever you're looking at helps, too, and "proves" to your brain that each eye really does correspond in the same direction and to the same space.
-Dr Greenwald has a method of using prisms to cause diplopia in ARC. I gathered that the reason is to show the brain that the ARC adaptation isn't going to work anymore, and that a new correspondence must be developed (NRC).
My situation
With my current understand of ARC, this is what I can say about my situation:
-I have a tendency to "paste" and have a panoramic view of the world, but with some activities I can bring things together.
-Sometimes I have diplopia "against the rule", and sometimes I don't.
-I really don't think that I have a faux-fovea or any faux-fusion. I have to grit my teeth and straighten my eyes to do anagylphic / flat fusion activities, and I'm certainly not able to fuse while maintaining a deviated eye.
-When I do the afterimage test, I get an ARC response that I can bring into an NRC response by blinking and looking at a bright light.
So, what is going on with me? Why am I ARC sometimes, yet NRC at other times? Is it possible to be both? Apparently, it is possible. From Strabismus and Amblyopia, by Donald J. Getz, O.D. (it's a wonderful book, by the way!):
Reading that certainly made me feel better. I just knew that there had to be a "both" option when it came to this correspondence stuff. I'm going to continue to work hard on my monocular and bi-ocular skills, until something magical happens, like recently happened with our friend Strabby.
I also hope that this post will be helpful for any other vision therapy patients who have read about ARC, and lay awake at night worrying about their correspondence status. Fear not!
-I have a tendency to "paste" and have a panoramic view of the world, but with some activities I can bring things together.
-Sometimes I have diplopia "against the rule", and sometimes I don't.
-I really don't think that I have a faux-fovea or any faux-fusion. I have to grit my teeth and straighten my eyes to do anagylphic / flat fusion activities, and I'm certainly not able to fuse while maintaining a deviated eye.
-When I do the afterimage test, I get an ARC response that I can bring into an NRC response by blinking and looking at a bright light.
So, what is going on with me? Why am I ARC sometimes, yet NRC at other times? Is it possible to be both? Apparently, it is possible. From Strabismus and Amblyopia, by Donald J. Getz, O.D. (it's a wonderful book, by the way!):
It is possible that correspondence will vary dependent on the conditions of the test. Often, some tests will indicate normal correspondence and other tests will indicate anomalous correspondence.
This above observation has led to the conclusion that what likely exists is a duality of correspondence. It is felt that what exists is an apparent anomalous correspondence with a latent normal correspondence. The most obvious example of this phenomenon is an intermittent exotrope who displays normal correspondence when the eyes are straight and anomalous correspondence when the eye is deviated. This is a relatively common observation.
Reading that certainly made me feel better. I just knew that there had to be a "both" option when it came to this correspondence stuff. I'm going to continue to work hard on my monocular and bi-ocular skills, until something magical happens, like recently happened with our friend Strabby.
I also hope that this post will be helpful for any other vision therapy patients who have read about ARC, and lay awake at night worrying about their correspondence status. Fear not!
Thanks, Dr. Press. I had read that normal/anomalous correspondence really happens in the brain, and not in the retina, and I certainly believe it. That's why I'm always talking to my brain when I'm doing my VT homework.
ReplyDelete"Hey brain. These things are located in the same space, so point your eyes there and start seeing it that way!"
I have strabismus and I'm 40 years old. I had corrective surgery when I was two, would there be any hope for improving my vision now? I'm pretty sure my vision switches between suppression and panoramic field. I've never had an eye doctor explain why I see the way I do as well as you just did. Most of them just dodge my questions or blow them off. I would love to improve my depth perception.
ReplyDeleteHi Josh,
ReplyDeletethank you so much for explaining this - it seems like the only explanations that exist are for professionals, not for the people affected.
I do think this is what I have. To make a long story short, I had a very large angle esotropia and started to develop lazy eye in childhood, but was treated and have since the age of 6 been alternating effortlessly. I also always felt I had great eyesight, never any trouble with dizziness, lack of focus or peripheral vision as described by Susan Barry in Fixing my Gaze. Was told that I could have surgery when I got older, for purely cosmetic reasons. At the age of 16 I wanted it, rather badly, but the day before surgery I went through a lot of tests and they looked rather surprised and worried and said we're sorry, can't do the surgery, it would ruin your eyesight. After lots of optometry they decided to correct it a bit, as much as was possible without causing permanent double vision - with prisms that corrected my eyes properly I was seeing two very clear double images with my right eye, while the left one (which is stronger) apparently suppressed. I didn't really try to understand what was going on at the time, but I assume now that the problem was anomalous correspondence and I developed exactly the double vision that the optometrists expected I would have. Thing is , if I focus, the second image becomes much less prominent and it never bothered me at all. Since they said nothing more could be done, I never bothered going to any second opinion or looking for additional treadment, it was just like adding pain to old wounds and I wanted to avoid that. But, now after almost 30 years, I went to another specialist and she says she thinks I should have surgery anyway since I can suppress the double image quite well especially with the left eye. It is very ironic though to feel you have great eyesight although one of your eyes is totally off upwards-inwards, and that the price of correcting it might be high. In my case, they also said my eye would probably go back to its corner position if they tried to correct it too much, or suppressed so much that it would go blind. I wouldn't have bothered with it today either unless it hadn't been such a massive social handicap. Now I want to try and challenge that "nothing can be done"-scenario as best as I can, including getting vision therapy after surgery to try to convince my brain to rewire. Thanks again for very well explained info :) and good luck with the excercises!
Hi Josh, This is wonderful stuff. However for a couple of reasons (problems that are mine and have nothing to do with your presentation) I'm having trouble following everything here (including replies.) So I'd like to ask two questions about just one aspect of this presentation.
ReplyDeleteIn this presentation you included the following:"Here's where it gets complicated. Instead of (or in addition to) suppression, the brain can alter the correspondence. Let's say that your left eye deviates 45 degrees outward. Your brain operates under the newer, more realistic assumption that your right fovea points straight ahead, and your left fovea points 45 degrees to the left. That is an abnormal or anomalous correspondence.In the case of exotropia, this can lead to a widened, panoramic visual field. Instead two eyes operating binocularly to make one image, the two eyes operate monocularly to make one panoramic image, neatly joined in the middle."-------I have two questions about this: 1) In a situation like mine (see below) where are the foveae?2) If I had surgery to align my eyes would I lose my "panorama?" (Note: The risk of double vision has been deemed to be extremely small for a couple of reasons.) Here's my situation: I am an alternating exotrope with excellent control and awareness regarding choice of which eye I'm "using." I have panoramic viewing that works with both eyes. (When "using" the right eye the left eye turns out and creates the panorama and visa-versa). The turn-out is about about 35 diopters in each eye when it's not being "used." Because of the degree of turn-out there is a small area of overlap where the two eyes see the same thing. I suppress that area. Note: I also have some suppression of the image from the eye that I'm not "using" but the image is still there and is useful to me.(I apologize if these questions have been asked and answered elsewhere. If they have, would you please direct me there? I also apologize if I am lacking information needed to discuss this issue in a useful way. If that's the case would you please suggest a good place to go for that?)Thanks!
I don't know why my post got all mis-formatted! Apologies. Hope you can sort it out. I may try to post again sometime and see if I can get it right.
ReplyDeleteHere is a piece that addresses Anomalous Correspondence. It lists and describes a variety of types of correspondence (which I've listed after the link). I am now even more confused and over-my-head that ever. But maybe this will help clarify the issue for others. -Frances
ReplyDeletehttp://arapaho.nsuok.edu/~salmonto/vs3_materials/Lecture26.pdf
I. Normal correspondence
II. Anomalous correspondence
A. Harmonious anomalous correspondence
B. Unharmonious
1. Unharmonious AC
2. Paradoxical AC, Type I
3. Paradoxical AC, Type II
Here is an piece with information about several kinds of Anomalous Correspondence. I'm now more confused and in-over-my-head than before. But perhaps this will help clarify the issue for others. (Below the link I've listed the different kinds of AC addressed.)
ReplyDelete-Frances
http://arapaho.nsuok.edu/~salmonto/vs3_materials/Lecture26.pdfI
Normal correspondence.
Anomalous correspondence
A. Harmonious anomalous correspondence
B. Unharmonious
1. Unharmonious AC
2. Paradoxical AC, Type I
3. Paradoxical AC, Type II
I have some questions related to the diagram that shows how the brain uses one false fovea and one true fovea to create depth perception.
ReplyDeleteIf the person has no depth perception (the brain is not using a false fovea) why can't the eyes be trained to converge and the brain be taught to fuse the images from the true foveae?
My reason for this question has to do with what my vision therapist told me about my goals.
She said that true depth perception is not a realistic goal for me (that it is "off the table"). She also told me that it might be possible for me to use my peripheral vision to create a sort of faint version of depth perception.
I am an alternating exotrope with panoramic viewing and no depth perception. I don't know if I have AC. (When I wear red/green glasses half the room is red and half is green. I have no fusion. I don't know if I have doplopia against the rule. I do remember a prism test that created diplopia but I don't know if it was crossed or uncrossed.)
Perhaps someone here can explain why I have to settle for a faint version of depth perception. My preference of course would be to get full depth perception via NC, but I might be willing to use AC and remain wall-eyed if necessary.
Oh and while I'm at it: Maybe someone has an idea about what it is that my therapist is aiming for. (What does she hope to get my eyes and brain to be doing in order to achieve this faint depth perception?)
Thanks,
Frances
OMG. Thankyou! Your experience is exactly like mine.
ReplyDeleteI've been working on vision therapy and have realised that sometimes my eye is exotropic, but I can still see out of it, I just have widened view, and the "stitching" in the middle is kind of weird. I can't really perceive it properly.
What is the thing you were talking about with Dr Greenwald and prisms? Got a link?
This is an insightful explanation about ARC and how it affects vision.
ReplyDelete